
Pathology Associated With Wisdom Teeth
When wisdom teeth (aka “3rd molars”) form we had only two choices before Zero3® TBA (3rd molar tooth bud ablation): either prophylactically extract these teeth in late teens or early 20’s – before roots fully form – or monitor and treat them as pathology develops later in life. These teeth are uniquely troublesome because they are the most frequent teeth to be partially or fully impacted (fail to erupt completely) with only 16% erupting normally. 1 This makes them extremely prone to trapping food and holding bacteria around their crown and root surfaces beneath the gum line. As a result, wisdom teeth are – by far – the single most likely teeth to have pathology associated with them and require repeated, expensive interventional treatment later in life at a rate of nearly 99%. 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12
This 34 year old patient has all four third molars present (circled) and fully erupted into occlusion. They appear disease free…but are difficult to keep clean. 3rd molars are the most likely teeth to decay or have gum disease with a >98% probability that decay and gum disease will occur around all four teeth over this patient’s life time.
To illustrate just how consistent wisdom tooth-related problems are for operations that employ people age 18 to 25 – such as the military – it has been reported that as many as 22% of all non-combat emergency department visits at U.S. military support facilities were related to dental problems, the most common being 3rd-molar related.16 The stated preference by all branches of the military is to have wisdom teeth removed – even if asymptomatic – prior to deployment into remote zones of active military operation.17 All retrospective studies conducted by the military demonstrated predictably high rates of infection leading to 3rd molar pericoronitis, the painful swelling and infection in the gums around wisdom teeth when they fail to fully erupt.18, 19 In battle zones 3rd molar pericoronitis “is fraught with difficulty…and of those that need to travel, 70% were moved by helicopter”.20
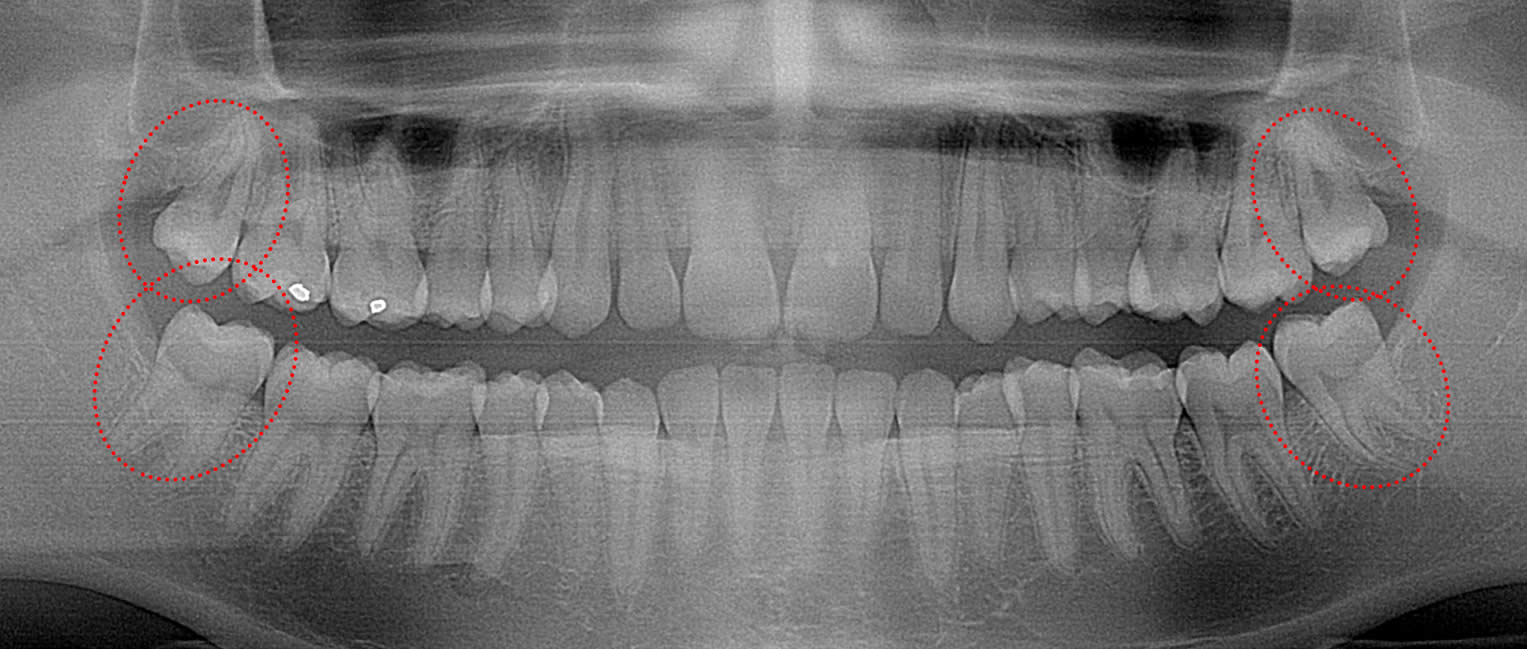
This 26 year old patient has all four 3rd molars present (circled). The upper right 3rd molar is badly decayed and the other three are partially erupted with signs of decay forming. Immediate extraction of all four is recommended.
In an extensive literature search conducted by Marciani it was concluded that less than 2% of middle-aged and older subjects with retained and visible 3rd molars were free of any history of decay or gum disease associated with their 3rd molars, mirroring the findings of numerous prior literature reviews.26

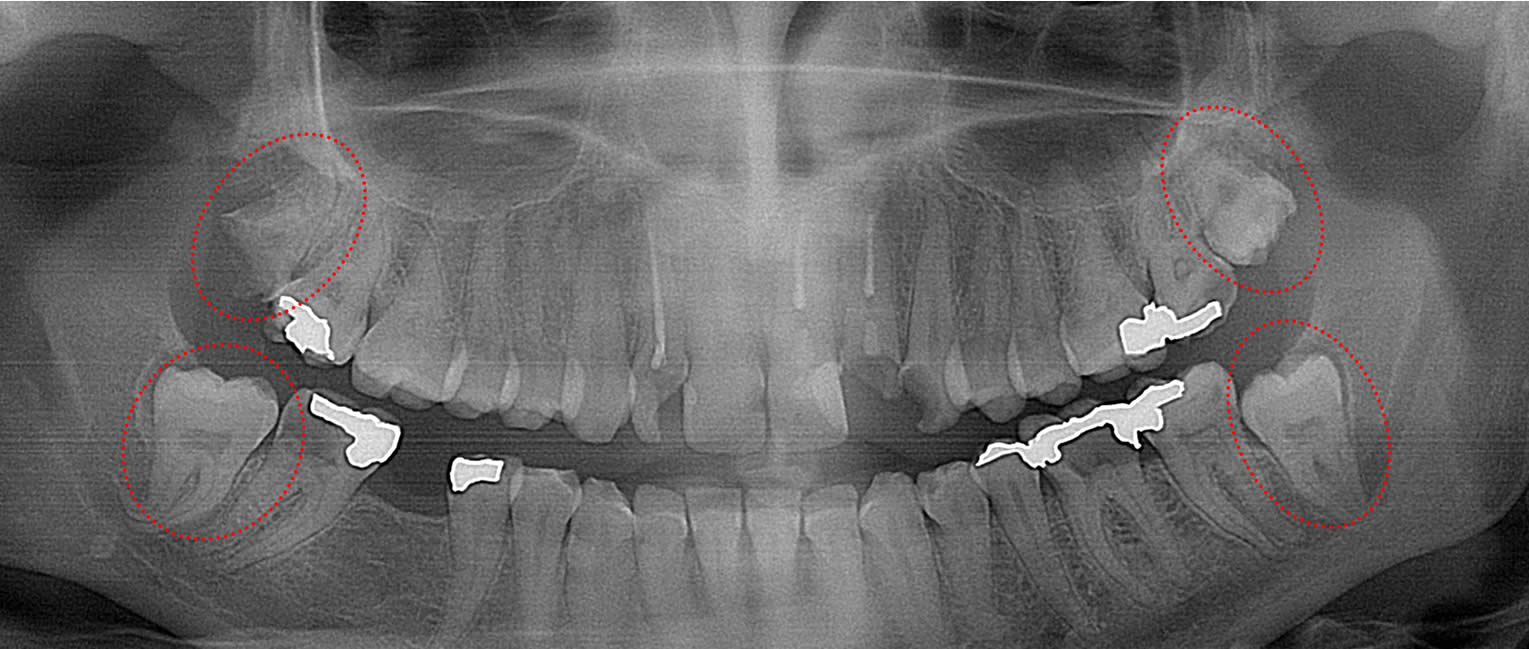
This 55 year old patient has bilateral mandibular 3rd molars with cysts forming around them (circled) that is destroying the bone in her mandible. This patient will likely lose her 2nd molars and suffer mandible fractures if the 3rd molars and cysts are not immediately removed.
Approximately 7% do not form wisdom teeth and have none of the problems described above. The goal of Zero3 TBA is to block wisdom tooth formation from ever starting, which will allow everybody that starts forming wisdom tooth buds to mimic those lucky few that never form these problematic teeth. We expect Zero3 TBA to be the safest and lowest cost alternative to prophylactic extraction in teens or waiting for problems to emerge later in life after wisdom teeth fully form.